Cognitive Behavioural Therapy
Cognitive-Behavioural Therapy for Chronic Health Conditions
Cognitive behavioural therapy (CBT) is a structured talking therapy that can help patients to accept and adjust as best they can to their condition. It can help improve recovery, ability to function and quality of life; and compliment well the work that you as a practitioner can offer.
When can talking therapies be indicated?
- Therapy can be particularly useful in helping patients cope better with some of the very real and frightening symptoms of PoTS (such as a racing heart, chest pain, and dizziness) in such a way that prevents any anxious responses to these sensations causing them to get worse.
- It can help patients cope better with the unpredictability of their illness.
- It can address stress that illness places on relationships with others.
- CBT can help if our mood is or has become low. When our mood is low, we often have distorted negative thoughts about ourselves, the world and the future. Unfortunately, people who experience PoTS are more likely to experience sleep difficulties, suicidal ideation and changes to their quality of life associated with depression.
- Patients with chronic illness are often facing a type of grief – a loss of a future that they had expected for themselves. They may have frustrations about the time before diagnosis when many patients are not believed or are misdiagnosed with conditions such as anxiety or panic disorder.
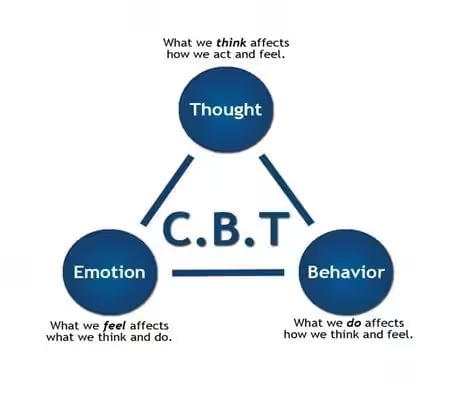
The CBT approach helps us understand that it is not the bare facts of a situation alone that causes how we end up feeling. Even when it comes to very genuinely difficult life-events, it is the way that we have learnt to think and respond to a situation that affects how we eventually feel. Our ways of thinking can become such habits that they feel like ‘the truth’; but with practise we can choose to notice these unhelpful patterns and to change them to help us feel better. In essence CBT aims to teach us to be a better friend to ourselves in terms of what we do and how we talk to ourselves.
“Are you suggesting it is all in my head?”
Clinical experience suggests that the referral to seek psychological support is often best received and taken-up by patients when it comes from a trusted healthcare provider actively involved in their care. Unfortunately, many patients prior to correct diagnosis have had their PoTS symptoms misdiagnosed, often as ‘all in their head’ (for example 50-80% of patients). As a consequence, a suggestion by a medical professional to seek psychological support can be misinterpreted by patients as a trivialisation and misunderstanding of the physical nature of their illness; leaving them reluctant to access this important form of support.
It can help to explain that just as patients with illnesses that are not caused by deconditioning may require input from physiotherapy services to prevent future deterioration and adjust to the changes wrought by their illness, so patients with illnesses not caused by psychological processes can benefit enormously from psychological support going forward. A sensitively discussed referral can help patients access this important part of their treatment package.
Some issues that could be addressed in CBT:
- Adjusting to the unpredictability of the illness
- Coping with scary physiological sensations
- Strategies for switching off flight/flight mode
- Managing pre-existing or associated anxiety or mood/adjustment disorders
- Grief associated with loss of health and life/ relationship changes
- Activity pacing
- Sleep difficulties
- Relationship difficulties
- Self-esteem and self-compassion
- Shaking off an illness-identity
- Acceptance and living optimally
What can a patient expect from CBT?
A good therapist should take time to help their patient understand how the treatment will work and identify their goals. In terms of behavioural changes this might include work towards accepting limitations, adjusting to the unpredictability of chronic illness, and helping with pacing to achieve the challenges of daily-living whilst still maintaining activities which most help us feel positive and fulfilled.
They should help patients become aware how thoughts or cognitions about having a long-term illness or disability, can influence our mood and even our symptoms.
Although there may not be many therapists who have experience working with PoTS, practitioners experienced in working with patients with other long-term health conditions should be able to adapt their approach usefully to a particular situation. A good clinician will take time to read relevant information to understand the condition. Inevitably a good collaborative mutli-disciplinary approach will yield the best outcome for all.
Finding a therapist
A patient’s General Practitioner should be able to advise them how to access a suitable NHS therapist or IAPT service in their area. The BABCP (British Association of Behavioural and Cognitive Psychotherapies) keeps a list of accredited therapists and has a search facility on their website. Psychologists should be registered with the Health Care Professionals Council.
Successful therapy is a lot about finding a therapist you feel comfortable with, so it is reasonable to take time to explore your condition together in detail, how that affects you specifically. This enables a formulation of your specific circumstances and an associated therapy plan. This collaboration can inspire mutual understanding and confidence and establish the foundations of an excellent working relationship.
Although everyone’s needs are different, a good CBT therapist can support patients in finding optimal ways to look after their mental and physical needs, getting them in the best shape to manage their unique symptom profile most effectively.
Does a psychology referral negate the need for a referral to a PoTS specialist?
Collaborative working is of course key. Health providers are increasingly recognising that the separation that we attempt to make between mental and physical health is unhelpful, and physical health practitioners are increasingly aware of the inevitable emotional and psychological strains on their patients’ health which standard healthcare is not equipped to address. Recent NHS initiatives Investing in emotional and psychological well-being for patients with long-term conditions (2011) and the Five Year Forward View for Mental Health,(2016) continue to prioritise and increase funding for psychological support for chronic and acute physical health conditions. The latter paper sets out plans for implementation of integration of services for mental health and long-term conditions and medically unexplained symptoms. There is no specific pathway yet for PoTS yet, but there are generic pathways for managing long term health conditions. Hopefully in the future physiological and psychological support will be routinely provided together.
We are yet to fully understand how trauma, inflammation, our genes, physiology, hormones, our gut microbiome, things that stress us, thoughts, expectations, social supports and other physiological and functional processes work together to determine our health outcomes and recovery. It is likely that there is a unique ‘illness thumbprint’ for everyone.
During the next decade ongoing research might hopefully bring us closer to some understanding – in the meantime it seems sensible to positively influence all the aspects of that complex process that are under our control.
As such it makes sense to enlist the support of an experienced therapist to optimise our patients’ behaviours and thinking patterns, reduce stressors, and prioritise and maximise their capacity to have rewarding relationships, interests and identity within.
Hopefully you can reassure your patients that they will continue to have your input, with a physical health lead and a mental-health lead both being part of a team they can trust; so that your patient can take the lead in co-ordinating and managing their illness positively.
Evidence for the benefits of CBT

There is very little published in medical journals about the effectiveness of CBT for PoTS. There are some case-reports, unpublished studies, and patient survey data that are suggestive of benefits to quality of life and functioning, and some good research being undertaken currently.
There is good and extensive evidence, however, on the effectiveness of CBT for other physical health conditions. The impact of chronic obstructive pulmonary disease (COPD) on quality of life has in research been equated with the impact of PoTS, and in both disorders, patients have to manage unpleasant physical symptoms which can be easily confused with, and escalated by, anxiety. The benefit of CBT with this population has been well evidenced. CBT has proved efficacious in terms of quality of life, treatment adherence, mood and even disease progression in physical health conditions including cancers, multiple scleroses and diabetes.
As evidence accrues that changing our thoughts can have a demonstrable influence on not just our brain-chemistry but also our physiology (and vice-versa) it seems increasingly sensible that improving our mental health can have an impact our physical heath.
What about other therapies?
Although CBT has been most extensively researched and is recommended by NICE guidelines as the first-choice psychological therapy for many physical health conditions, other types of treatment can also be beneficial. To a certain extent therapy approach is a matter of individual preference.
Many CBT practitioners also incorporate ‘third-wave’ therapies such a mindfulness-based CBT, Acceptance and Commitment therapies and Compassion-focused approaches. As they are new, evidence about their effectiveness is limited. However, it is clear that meditation and mindfulness (being fully present, in the moment, with acceptance), can have profound effect not just on stress-management and energy-levels but also on physiological processes including blood-pressure, heart-rate, blood sugar regulation and even a measurable effect at the cellular level in cancer patients.
Will CBT work for my patient?
To recap the full benefit of therapy generally requires a patient to be committed to engaging fully in sessions and tasks between sessions, to have some hope or confidence in the approach, and, guided by their therapist, be able to gain good insight into the consequences of their thinking styles and behavioural patterns.
It can be very hard-work making all the necessary life-changes to live with PoTS. It can help patients to know that after that hard work, and adjusting to what they cannot do, while focusing on what they can do, that many patients with PoTS report enjoying happy and fulfilling lives.
As with many long-term health conditions, although we would not ever wish them upon ourselves or others, a positive outcome can be a new appreciation for the things that really matter; and an opportunity to re-establish priorities, and live life thereafter to our full potential.
Share this page
This information is general information about PoTS and is not an alternative to medical advice from your doctor or other healthcare professional. You must always consult your doctor or healthcare professional.
Last review 01-10-2021
Next review 01-10-2024
Version 2